-
Imaging is brain ต้องเร็วเพราะรักษา prenumber (สมองส่วนที่กำลังจะขาดเลือด) ก่อนที่จะไปเป็น core infarction
-
CT brain ควรรีบทำเพื่อ specific treatment (IV-rtPA เปิดเส้นเลือดส่วนกลางได้ดี)
-
Endovascular thrombectomy พิจารณาทำเพื่อเปิดหลอดเลือดส่วนต้น (CTA หลัง IV rtPA)
-
มาหลัง 6 hr ต้องทำ CT prefusion imaging > thrombectomy
Pre-hospital management
-
Home Education program > activation 1669 > EMS > hospital (Telemedicine)
Stroke scale

-
NIHSS score
-
0 = No, 0-4 = Minor stroke, 5-15 = Moderate stroke, 16-20 = Mod to severe stroke
-
Head and Neck imaging
-
NC CT brain (exclude ICH before IV alteplase)
-
MRI: ใช้เวลานาน, EWI (core infarct), flare (เกิน 4 hr), เห็นได้ดีใน posterior circulation/ early onset/
* unclear onset (น้อยกว่า 4.5 hr,18-80 yrs c good ADL) เพื่อดู DWI-flare mismatch [WAKEUP18]
เพื่อพิจารณา IV alteplase (IIa)
-
DWI < 1/3 MCA = no hemorrhage + ไม่มี flare (mismatch) พิจารณา rtPA
-
ถ้าเกิน > 1/3 หรือ Match (มี DWI/flare) เกิน 4.5 hr มีโอกาส hemorrhage ไม่ให้ rtPA
-
* MRI fast track (1-10 CMBs microbleed จุดเลือดออก) ให้ IV rtPA ได้ แต่ถ้า >10จุด = ICH มากขึ้น
IV rtPA (Alteplase) Criteria
-
Onset < 4.5 hrs
(รวมถึง 3-4.5 hr + age>80, on warfarin (INR <1.7), hx of 3mo stroke and DM)
จะไม่ให้เมื่อ (ไม่ได้ประโยชน์) > 3 hr + very severe stroke (NIHSS score > 25)
มี large vessel occlusion และนาน clot จะยาว ใช้ medical มักเปิด vessel ไม่ได้
-
Age > 18 yrs
-
BP < 185/110 mmHg (BP shoot เสี่ยงเลือดออก reperfusion hemorrhage)
-
Severe or minor with disabling + in 3 hrs
-
Glucose > 50 mg/dl
-
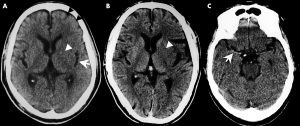
CT scan: early ischemic changes on NCCT (hyperdense MCA, loss of ribbon sign)
-
> 1/3 MCA : High risk for bleed post rtPA (=1/3 ยังให้ได้)
-
> 2/3 MCA : large infarction (Frank hyperdensity)
-
3/3 MCA : Malignant infarction
-
-
Prior antiplatelet
-
Monotherapy ให้ rtPA ได้
-
Combination (DAPT=ASA/plavix) ยังให้ได้แต่เสี่ยง ICH มากขึ้น
-
-
Preexisting disability ต้องคุยเรื่องความคุ้มค่าอีกที
-
ESRD on H/D ให้ rtPA ได้เมื่อ normal aPTT
-
Seizure at onset ให้ได้ แต่ weak จาก gross paralysis or postictal และต้อง R/O ICH ก่อน
-
Extracranial cervical dissection, unruptured intracranial aneurysm ให้ได้
-
Stroke mimics ไม่มี organic ชัดเจน ให้ได้
-
Menstruation ให้ได้ ยกเว้น serious bleeding
-
Pregnancy พิจารณาเป็นรายๆ ไป ต้องระวัง venous stroke, eclampsia, และโอกาส ICH มาก
-
Acute MI หรือ recent MI (ยกเว้น large extensive wall) สามารถให้ rtPA (V/S stable) ก่อนแล้ววทำ CABG ถ้าไม่ stable > resuscitate + PCI ก่อน (ต้อง save heart ก่อน)
ASPECTS score (Alberta stroke program early CT score)
-
คะแนนโอกาส bleed หลังได้ rtPA
-
10 pts = normal CT (เหมือนกันทั้ง 2 ข้าง), <6 pts = high risk for post rtPA bleed/ contra for MT (4 รอยคล้ำ), 0 pts = entire MCA (malignant MCA)
Hypertensive management in pts rtPA
BP > 185/110 mmHg
-
Labeteral 10-20 mg IV, repeat x1
-
Nicardipine 5 mg/hr, titrate q 5-15 mins to max of 15 mg/hr
Maintain BP < 180/105 mmHg during and after rtPA
-
Monitor BP q 15mins for 2 hr, q 30mins for 6 hrs, then q 1hr
-
If SBP > 180-230 mmHg or DBP > 105-120 mmHg
-
Labetalol 10 mg IV then drip
-
Nicardipine drip
-
IV Nitroprusside
-
Minor stroke (0-5 pts)
-
Minor c disabling in 3 hrs > ให้ IV rtPA ได้ประโยชน์เพราะอาจ progress ได้
-
Minor c disabling in 3 – 4.5 hrs > ให้ IV rtPA ได้
-
Minor c non-disabling (ไม่มีอาการ) > ไม่ให้ IV rtPA
-
[PRISM2018] rtPA vs ASA(300) ใน minor with non-disabling > outcome ไม่ต่างกัน
-

IV rtPA (Alteplase) Contraindication
-
Onset ชัดเจน > 4.5 hr
(Unclear onset + symptoms recognize < 4.5 hr >> MRI [WAKEUP2018])
-
Patient Past illness
-
Ischemic stroke < 3mo (อาจจะพิจารณาให้บางเคส)
-
Acute/severe head trauma < 3mo
-
Intracranial/intraspinal surgery < 3mo
-
Hx of ICH (spontaneous, idiopathic)
-
GI malignancy, Active GI bleed <21day
-
IE-mycotic aneurysm (ไข้ ฟัง murmur ก่อนให้), Aortic dissection,
Brain tumor (intra-axial)
-
-
Investigation
-
NC CT: seen hemorrhage, large acute hypodense
-
Plt < 100,000 / INR > 1.7 / aPTT > 40 secs / PT > 15 secs
-
-
Medication
-
Full-dose LMWH (Enoxa) <24hr
-
Thrombin, Factor Xa inhibitors (NOACs) <48hr
-
Abciximab !
-
IV aspirin <90min
-
IV Alteplase dose
-
0.9 x BW (10% bolus, 90% drip in 60 mins + monitor)
[E-CASS4 Extend 2019] อาจจะมีประโยชน์แนวโน้มให้ 4.5 – 9 hr ได้
Post rtPA bleeding
-
Stop rtPTA
-
CBC, PT, PTT, INR, fibrinogen level, G/M
-
CT brain
-
Cryoprecipitate (factor VIII) 10U IV 10-30 min
onset: 1hr, peak: 12hrs
additional dose for fibrinogen level < 200 mg/dL
-
Tranexamic acid 1000 mg IV 10 min then 10 mg/kg x3-4/d until control
peak: 3hrs
-
Consult Hemato, NeuroSx
-
Control BP, DTX